Development of a Tumor Marker Gene Model
–Toward Better Surgical Decision-Making for Patients with Advanced Pancreatic Cancer–
Key Points
- Pancreatic cancer is frequently diagnosed at an advanced stage and has one of the lowest survival rates among all cancers.
- In addition to chemotherapy and radiotherapy, performing surgery at the appropriate timing is critical.
- Tumor markers are helpful for determining surgical eligibility, but individual variability has posed a challenge.
- This study demonstrates that combining tumor markers with genetic types can serve as a useful indicator for surgical decision-making.
Summary
A research group led by Assistant Professor Haruyoshi Tanaka, the Department of Surgery, Nagoya University; graduate student Ayano Sakai, the Department of Surgery and Science, Faculty of Medicine, Academic Assembly, University of Toyama; Dr. Masaya Suenaga, Chief Surgeon, the Department of Surgery, Nagoya Medical Center, National Hospital Organization; Professor Tsutomu Fujii, Toyama University; Professor Tomoki Ebata, Department of Surgery, Nagoya University; and former Professor Yasuhiro Kodera, Nagoya University, has developed a novel prognostic model applicable to advanced pancreatic cancer.
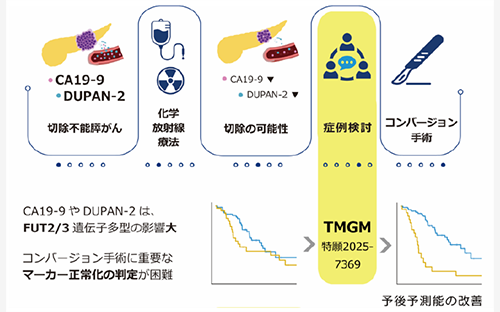
Pancreatic cancer is often detected at an advanced stage and is associated with poor prognosis. Treatment usually involves a multidisciplinary approach that combines chemotherapy, radiotherapy, and surgical resection at an optimal time. Tumor markers such as CA19-9¹ and DUPAN-2² are commonly used to assess the appropriateness and timing of surgery, but their values vary significantly between individuals, making evaluation difficult.
In this study, the researchers focused on the relationship between tumor marker levels and the genotypes of FUT2³ and FUT3⁴ and analyzed the changes in marker levels following preoperative chemotherapy or radiotherapy by genotype. They found that the variation in CA19-9 and DUPAN-2 levels was more strongly associated with the FUT2/3 genotype than with disease severity based on the resectability classification⁵.
Based on this finding, the team developed a new prognostic model for patients who were initially diagnosed as unresectable but became eligible for surgery following treatment. This model integrates CA19-9, DUPAN-2, and FUT2/3 genotypes into a unified predictive tool, referred to as the tumor marker gene model (TMGM). Compared with conventional models that rely solely on standard reference values for tumor markers, TMGM demonstrated significantly superior predictive accuracy for patient survival.
This study suggests that using TMGM as a guide for surgical decision-making could help avoid unnecessary surgeries with limited benefit and may offer surgical opportunities to patients previously deemed ineligible. The results of this study will be published in the British Journal of Surgery on April 29, 2025.
Research Background
Pancreatic cancer is one of the most lethal malignancies and is often diagnosed at a stage when surgical resection is no longer feasible. Treatment strategies are determined based on resectability classification, but many patients are already beyond the scope of curative surgery at diagnosis. However, recent advances in chemotherapy, radiotherapy, and multimodal treatment approaches have gradually improved outcomes.
Surgical resection remains the only curative option, capable of removing visible tumors in a single procedure. However, it imposes a heavy burden on the body and precludes concurrent treatments, making proper timing essential. Imaging modalities such as CT, along with tumor markers like CA19-9 and DUPAN-2, are used to guide surgical decisions. Yet, there is no definitive standard for determining optimal timing or benefit of surgery, and decisions are typically made through multidisciplinary discussions among specialists. Due to inter-individual variability in tumor marker levels, assessing these markers remains challenging.
To address this issue, the research team led by Assistant Professor Tanaka examined whether individual differences in tumor marker levels could be attributed to genetic polymorphisms in FUT2 and FUT3, aiming to establish a new decision-making tool for surgical indication and timing.
Research Results
By performing polymerase chain reaction of DNA from pancreatic cancer patients who underwent surgery following preoperative therapy, the team successfully determined FUT2/3 genotypes in 341 out of 345 patients. Surprisingly, analysis revealed that changes in CA19-9 and DUPAN-2 were only mildly associated with resectability classification, whereas significant differences were observed when grouped by FUT2/3 genotypes .
Focusing on 88 patients initially diagnosed as unresectable (UR) who subsequently underwent surgery due to favorable treatment response, the team found that approximately 30% had rare genotypes such as FUT2-null⁶ or FUT3-null⁷. These patients exhibited markedly different survival outcomes compared to those with common genotypes.
These findings led the researchers to hypothesize that current evaluations based on tumor marker levels may be inadequate for patients with rare genotypes. They constructed the tumor marker gene model (TMGM) by incorporating FUT2/3 genotypes alongside CA19-9 and DUPAN-2. When applied to patients in the UR category, TMGM significantly outperformed conventional models in predicting survival.
This indicates that relying solely on tumor marker normalization may have led to surgeries with minimal benefit, or conversely, the missed opportunity for surgery in patients who were actually improving.
Research Summary and Future Perspective
Incorporating TMGM as a tool for determining surgical eligibility during chemotherapy or radiotherapy may help avoid surgeries with limited efficacy and identify patients who could benefit from surgery despite initial inoperability.
However, TMGM cannot yet be implemented in routine clinical practice for two main reasons:
1.The diagnostic reagents used in this study were developed solely for research purposes.
2.The study was retrospective in nature, based on post-treatment analysis.
To enable the widespread clinical use of TMGM, the following steps are necessary:
1.Development and regulatory approval of a genetic test kit for FUT2/3 polymorphism detection.
2.Conduct of clinical trials to validate the effectiveness of TMGM in a broader patient population.
The team plans to advance research on test kit development and initiate clinical trials to verify the utility of TMGM in real-world settings.
Glossary
1.CA19-9 (Carbohydrate Antigen 19-9): A widely used tumor marker that reflects tumor burden. It is measured using an NS19-9 antibody developed from a human colorectal cancer cell line.
2.DUPAN-2: Another major tumor marker, used alongside CA19-9. It is measured using a DUPAN-2 antibody derived from a human pancreatic cancer cell line.
3.FUT2 gene (Fucosyltransferase 2): A gene encoding an enzyme involved in the secretion of Lewis blood group antigens into bodily fluids.
4.FUT3 gene (Fucosyltransferase 3): A gene responsible for determining Lewis blood group types through fucosylation.
5.Resectability Classification: An imaging-based classification used in addition to cancer staging, assessing the feasibility of surgical resection. Categories include Resectable (R), Borderline Resectable (BR), and Unresectable (UR).
6.FUT2-null (F2N): A genotype in which both FUT2 alleles carry mutations (homozygous mutation), resulting in loss of FUT2 protein function. This condition is not directly linked to increased cancer risk.
7.FUT3-null (F3N): A genotype with homozygous mutations in FUT3, leading to loss of protein function. This condition does not directly increase susceptibility to pancreatic cancer or other diseases.
Publication
Journal
British Journal of Surgery
Title
FUT2 and FUT3 specific normalization of DUPAN-2 and Carbohydrate Antigen 19-9 in preoperative therapy for pancreatic cancer: a multi-center retrospective study (GEMINI-PC-01)
Authors
Haruyoshi Tanaka1,2,†, Ayano Sakai2,†, Masaya Suenaga3, Masamichi Hayashi1, Tomohisa Otsu1, Nobuhiko Nakagawa1, Keisuke Kurimoto1, Mina Fukasawa2, Kazuto Shibuya2, Nobuyuki Watanabe1, Masaki Sunagawa1, Junpei Yamaguchi1, Takashi Mizuno1, Toshio Kokuryo1, Hideki Takami1, Tomoki Ebata1, Tsutomu Fujii2, Yasuhiro Kodera1
1) Department of Surgery, Nagoya University Hospital, Nagoya, Japan
2) Department of Surgery and Science, Faculty of Medicine, Academic Assembly, University of Toyama, Toyama, Japan
3) Department of Surgery, NHO Nagoya Medical Center, Nagoya, Japan
†) Contributed equally to this work